
Revenue Cycle Management in Medical Billing: Why Most Practices Are Losing Revenue Without Realizing It
Revenue does not disappear overnight. It erodes slowly, predictably, and repeatedly.
And in today’s reimbursement environment, revenue cycle management in medical billing has become the difference between sustainable growth and silent financial compression.
For many healthcare organizations, billing is still treated as an administrative task.
It is not. It is a financial intelligence system or it should be.
This article examines the true state of revenue cycle management in medical billing, where revenue is leaking, why traditional billing models are failing, and how AI-driven revenue intelligence is redefining financial performance.
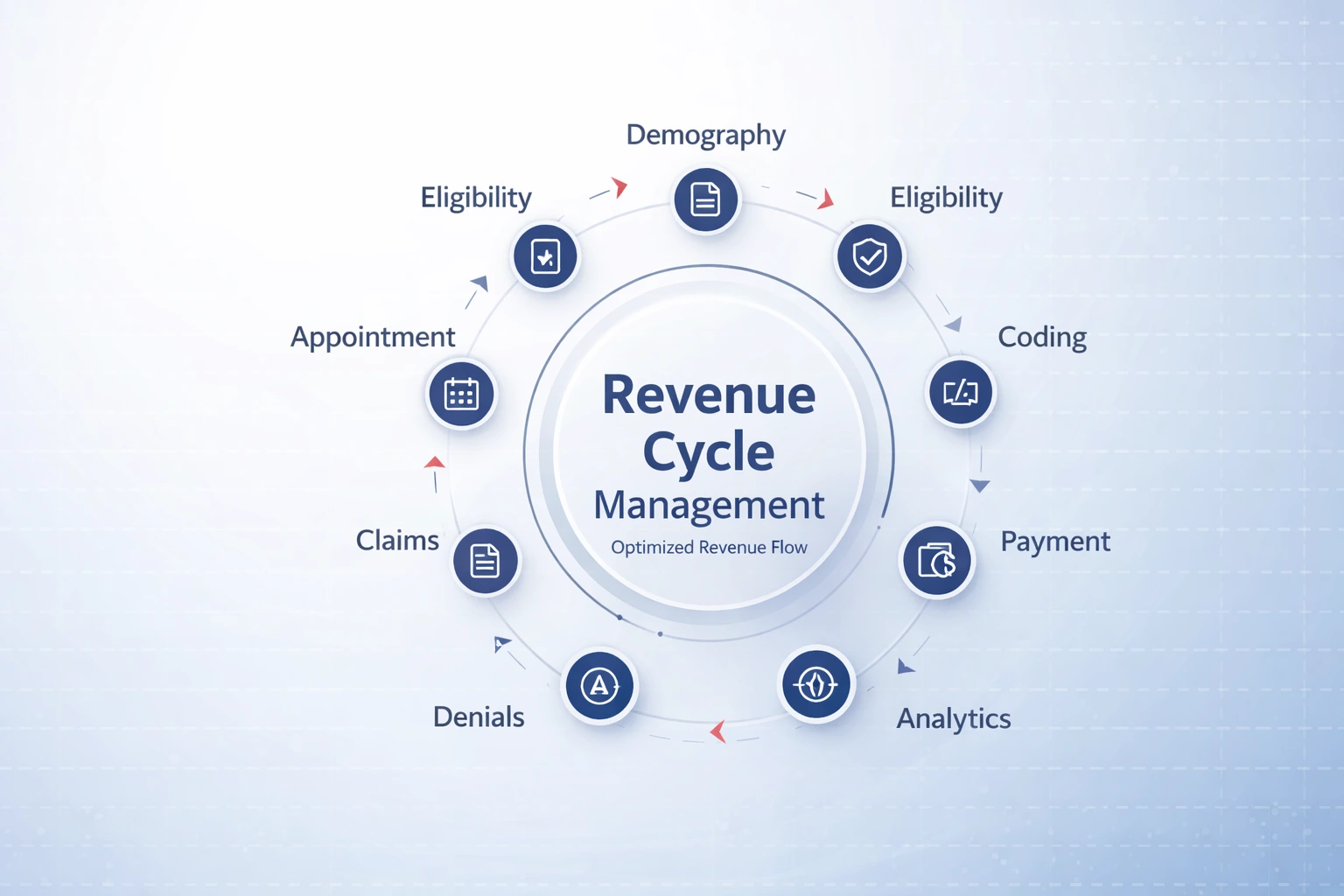
What Revenue Cycle Management in Medical Billing Actually Means
1) Patient intake and demographics
This is where revenue accuracy is either engineered or silently compromised.
Patient intake is the capture of identity, coverage, and billing-critical details at the front door. The goal isn’t “getting the patient in.” The goal is building a claim-ready record that will survive payer editing, clearinghouse logic, and patient billing.
What this step includes
- Collecting and validating patient identifiers (name, DOB, address, phone, email)
- Capturing subscriber vs patient relationship and guarantor details
- Confirming payer details (payer name, plan type, member ID, group number)
- Recording referring provider info when required
- Collecting consent forms and financial policies
Why it matters financially (not clinically)
- Incorrect demographics create downstream rework, delayed billing, and patient statement confusion.
- One wrong digit in a member ID can turn a clean clinical encounter into a billing fire drill.
Operational best practices
- Use standardized intake checklists (not “whatever the front desk remembers today”)
- Validate data in real time (format checks, duplicates, coverage format rules)
- Make intake “claim-ready,” not “visit-ready”
2) Eligibility and benefits verification
Eligibility is the financial gatekeeper. It answers: Is this patient covered today, for this service, at this location, under this provider and what will it actually pay?
Eligibility verification is not a checkbox. It’s benefits intelligence.
What this step includes
- Confirming active coverage on date of service
- Verifying in-network vs out-of-network status
- Identifying copay, deductible, coinsurance, out-of-pocket status
- Checking coverage limitations (visit limits, therapy caps, imaging rules, etc.)
- Confirming PCP/referral requirements where applicable
Why it matters financially
This step directly affects:
- whether you should collect at check-in
- whether the patient should sign an ABN/financial waiver (when relevant)
- whether the service should be rescheduled, re-routed, or pre-cleared
It prevents “surprise billing” scenarios that turn into patient disputes and write-offs.
Operational best practices
- Verify eligibility 48–72 hours pre-visit and again day-of for high-risk payers
- Convert benefits into a patient responsibility estimate (even if it’s a range)
- Route high-deductible plans into upfront collections workflows
3) Prior authorization management
Authorization is capacity control + revenue control. It ensures the payer has approved the service before it happens (when required).
This is not just admin work. It’s a documented approval pathway tied to service type, diagnosis, location, and rendering provider.
What this step includes
- Determining whether auth is required (payer + CPT + place of service rules)
- Submitting clinical documentation packages (notes, imaging results, orders)
- Tracking auth status, validity dates, and visit/unit counts
- Linking the auth reference number to the claim and documentation set
- Managing re-authorizations for ongoing care (PT, behavioral health, imaging, etc.)
Why it matters financially
- Auth touches scheduling efficiency (fewer reschedules), provider productivity, and cash predictability.
- Poor auth workflows create capacity waste: providers deliver care that becomes difficult to monetize.
Operational best practices
- Build payer-specific auth checklists by CPT category
- Centralize auth tracking (not scattered across emails and sticky notes)
- Tie auth to scheduling: no auth, no slot (for services where required)
4) Medical coding and claim submission
This is where clinical documentation becomes a payer-recognizable financial transaction.
Coding is not “assigning a CPT code.” It’s translating the encounter into:
- services performed
- medical necessity narrative
- correct bundling/modifier logic
- proper diagnosis linkage
- place-of-service alignment
- provider credential alignment
What this step includes
- Assigning CPT/HCPCS and ICD-10 codes based on documentation
- Applying modifiers accurately (e.g., 25, 59, TC/26, RT/LT, etc.)
- Ensuring correct place of service and provider identifiers (NPI, taxonomy)
- Running claim edits (scrubbers) before sending
- Submitting claims to clearinghouse/payer and monitoring acceptance
Why it matters financially
- Coding quality determines whether you capture the full value of the visit/procedure.
- “Claims submitted” is not the finish line. “Claims accepted cleanly and paid accurately” is.
Operational best practices
- Use specialty-specific coding playbooks (generic rules break in specialty workflows)
- Implement pre-submission quality checks (edit resolution before the payer sees it)
- Separate “charge entry speed” from “coding accuracy” metrics
5) Payment posting
Payment posting is where collections become truth in the system.
It’s not just entering payments. It’s reconciling payer logic, patient responsibility, adjustments, and contractual allowances so AR reflects reality.
What this step includes
- Posting ERA/EOB payments accurately at the line level
- Applying contractual adjustments and patient responsibility correctly
- Identifying payment variances (allowed amount vs expected)
- Handling secondary claims and coordination of benefits workflows
- Ensuring refunds/recoupments are correctly tracked
Why it matters financially
- Bad posting creates fake AR, distorted reporting, and incorrect patient billing.
- If posting is wrong, every KPI downstream becomes unreliable: days in AR, net collections, write-offs, patient balances.
Operational best practices
- Reconcile posting with contracts and fee schedules (where possible)
- Separate adjustment types clearly (contractual vs write-off vs administrative)
- Monitor posting lag time slow posting = delayed follow-up = delayed cash
6) Accounts receivable (AR) follow-up
AR management is the discipline of converting open balances into cash systematically, not emotionally.
AR follow-up is not “calling payers.” It’s structured work-queue execution with prioritization.
What this step includes
- Segmenting AR by payer, age bucket, balance size, and claim type
- Prioritizing high-impact accounts (large balances, time-sensitive claims)
- Performing payer follow-up, documentation resubmission, and corrections
- Managing patient AR: statements, payment plans, outbound collections pathways
- Tracking timely filing limits and escalation pathways
Why it matters financially
- Most AR problems are workflow problems upstream but AR follow-up is where cash is recovered.
- Without prioritization, teams waste time on low-dollar accounts while high-value balances age out.
Operational best practices
- Build AR work queues based on financial impact (not just date order)
- Use payer-specific call and escalation playbooks
- Track “touch effectiveness” (contacts that move claims forward vs busywork)
7) Denial management and appeals
This stage exists because payers frequently require additional steps to finalize reimbursement documentation requests, clarifications, coding corrections, or formal disputes.
What this step includes
- Categorizing issues by root cause (front-end, coding, contract, documentation)
- Standardizing resubmission vs appeal pathways
- Building payer-specific documentation packets and timelines
- Tracking outcomes and cycle times (what gets resolved, how fast, and why)
Why it matters financially
- Resolution management protects cash velocity.
- It also creates feedback loops: the only way to stop repeating problems is to classify and trend them.
Operational best practices
- Treat issues as datasets (clusters), not one-off fires
- Build repeatable appeal templates and evidence checklists
- Measure overturn/resolve rate and time-to-resolution, then improve upstream steps
8) Revenue reporting and analytics
This is where revenue cycle management in medical billing becomes an executive function instead of a back-office task.
Reporting should not be “here are your collections.” Reporting should answer:
- What’s slowing cash?
- Where is performance drifting?
- Which payers are compressing reimbursement?
- What workflows are failing upstream?
- What should we change this week?
What this step includes
- KPI dashboards (first-pass acceptance, net collections, days in AR, AR aging, variance tracking)
- Trend analysis by payer, provider, location, and service line
- Patient responsibility trends (bad debt risk, upfront collections performance)
- Operational productivity metrics (touches per FTE, resolution cycle time)
- Forecasting cash based on AR composition and payer behavior
Why it matters financially
- Without analytics, you can’t manage performance only react to symptoms.
- Revenue cycle becomes a monthly surprise instead of a controlled system.
Operational best practices
- Tie KPIs to action: every metric should map to a workflow owner and intervention
- Separate “volume metrics” from “quality metrics” (more claims ≠ better outcomes)
- Use benchmarks and internal baselines to spot drift early
The dangerous assumption: “Claims are being submitted, so it’s working.”
Most practices stop measuring at submission because submission is visible.
But submission is not optimization.
A revenue cycle can submit claims all day and still under-collect, mis-post, mis-estimate patient responsibility, let balances age, and lose forecasting accuracy.
A functioning revenue cycle is not defined by activity.
It’s defined by controlled outcomes:
- predictable cash flow
- accurate patient responsibility
- clean, timely reimbursement
- reliable financial reporting
- measurable performance improvement
The Financial Reality: Where Revenue Is Actually Lost
Healthcare leaders often monitor total collections.
Few monitor structural leakage.
In modern revenue cycle management in medical billing, revenue is lost in four primary areas:
1️⃣ Preventable Denials
Industry averages show initial denial rates between 10% and 20%, depending on specialty and payer mix.
Common denial triggers include:
- Authorization failures
- Eligibility errors
- Incorrect modifiers
- Diagnosis-to-procedure mismatches
- Medical necessity documentation gaps
High-performing systems aim for:
- First-pass claim acceptance rate: 95–98%
- Denial rate: Under 5–8%
Anything above that range represents preventable margin erosion.
2️⃣ AR Aging & Cash Flow Delays
Accounts receivable is the pulse of revenue cycle management in medical billing.
When:
- AR > 90 days exceeds 20–25%
- Days in AR surpass 50 days
You are not facing a collections issue.
You are facing a structural workflow failure.
Mature revenue cycles target:
- AR > 90 days: Below 15%
- Days in AR: 30–40 days
- Net collection rate: 95%+ of adjusted charges
Aging AR compresses cash flow and distorts financial forecasting.
3️⃣ Underpayment & Contract Variance
Most practices track denials. Few track underpayments.
Payers frequently reimburse below contracted expectations due to:
- Fee schedule misapplications
- Silent downgrades
- Bundled CPT reinterpretations
- Modifier suppression
- Incorrect payment logic
Without CPT-level variance analysis, underpayment remains invisible.
Revenue cycle management in medical billing must include contract-aware reimbursement auditing not just claim submission.
4️⃣ Inefficient Denial Appeals
Appeals are often handled manually.
They lack:
- Structured root cause clustering
- Payer-specific escalation strategies
- Tracking of overturn rates
- Measurable appeal cycle time
High-performing RCM operations measure:
- Denial overturn rate
- Average time to appeal resolution
- Repeat denial patterns
Reactive follow-up cannot compete with predictive prevention.
Why Traditional Billing Models No Longer Work
Many billing companies operate with a simple model:
Submit claims → Fix rejections → Send reports → Repeat.
What is missing?
- Payer behavior modeling
- Denial pattern analysis
- Underpayment detection
- Predictive AR prioritization
- Revenue leakage identification
Modern revenue cycle management in medical billing requires analytical depth.
Without analytics, billing becomes administrative not strategic.
AI Is Changing the Economics of Revenue Cycle Management
The most significant shift in revenue cycle management in medical billing is the integration of artificial intelligence.
AI-driven systems allow practices to move from reactive correction to proactive protection.
Key AI Applications Include:
- Predictive denial modeling
- CPT-level underpayment detection
- Payer-specific reimbursement variance tracking
- AR risk forecasting
- Work queue prioritization algorithms
- Revenue gap analysis against industry benchmarks
The measurable impact:
- 8–18% increase in net collections
- 15–30% denial rate improvement
- 25–40% reduction in AR > 90 days
- Improved first-pass acceptance rates
This is not automation for convenience. It is structural revenue optimization.
Specialty-Specific Risk in Medical Billing
Revenue cycle management in medical billing must adapt to specialty complexity.
Radiology
- Professional vs technical billing errors
- High-volume modifier sensitivity
- Authorization exposure
- LCD/NCD medical necessity scrutiny
Clinical & Molecular Labs
- Frequency limitations
- Policy-driven denials
- High-dollar CPT variance
- Payer-specific coverage restrictions
Behavioral Health
- Time-based coding accuracy
- Telehealth reimbursement shifts
- Authorization lapses
- Recurring small-dollar denial accumulation
Generic billing approaches fail under specialty nuance. Precision matters.
Compliance: Revenue Protection Through Governance
Revenue optimization without compliance discipline creates legal risk.
Modern revenue cycle management in medical billing must operate within:
- HIPAA compliance standards
- Business Associate Agreements (BAA)
- Role-based system access
- Encrypted communication channels
- Cybersecurity oversight
Compliance is not an add-on. It is embedded into financial operations.
KPIs That Define High-Performance Revenue Cycle Management
Practices serious about optimizing revenue cycle management in medical billing track:
- Gross charges
- Net collections
- Collection rate (% of charges)
- First-pass acceptance rate
- Denial rate and overturn rate
- Days in AR
- AR > 90 days
- Average appeal resolution time
Monthly KPI dashboards should reveal trends not just totals. Revenue intelligence requires visibility.
Why Redfort RCM Is Built for Modern Revenue Cycle Management in Medical Billing
Revenue compression is not solved by hiring more billers. It is solved by building a smarter system.
Redfort RCM positions itself as:
- ✔ A technology-enabled, AI-driven revenue optimization partner
- ✔ Not “just another billing company”
- ✔ Focused on measurable financial performance
What Makes Redfort Different
1️⃣ AI-Driven Revenue Intelligence
Redfort applies:
- CPT-level underpayment detection
- Payer-specific reimbursement variance tracking
- Denial pattern clustering
- Predictive AR risk modeling
This is aligned with the core promise:
Not reporting what happened but identifying what you're losing.
2️⃣ Full-Spectrum Revenue Control
Redfort delivers end-to-end revenue cycle management in medical billing, including:
- Appointment scheduling & intake support
- Eligibility & benefits verification
- Coding & billing
- AR follow-up
- Denial management & appeals
- Credentialing & payer enrollment
- MIPS participation & reporting
Revenue is managed holistically, not in fragments.
3️⃣ Specialty-Focused Precision
Redfort prioritizes high-complexity specialties such as:
- Radiology
- Clinical & Molecular Labs
- Behavioral Health
Workflows are built around specialty-specific denial risk and payer compression patterns.
4️⃣ Measurable Performance Targets
Redfort aligns optimization around benchmark-driven outcomes:
- 95–98% first-pass acceptance
- 8–18% lift in net collections
- 25–40% reduction in AR > 90 days
- 15–30% denial improvement
Performance is measured monthly through dashboards and executive reporting .
5️⃣ Compliance & Security Oversight
All operations are HIPAA-compliant, supported by Business Associate Agreements and cybersecurity oversight through Redfort Technologies .
Revenue protection includes data protection.
Final Thought
Revenue cycle management in medical billing is no longer a clerical process.
It is:
- Denial prevention
- Underpayment detection
- AR acceleration
- Contract enforcement
- Predictive financial modeling
Practices that continue using transactional billing models will experience increasing margin compression.
Practices that adopt AI-driven revenue intelligence will protect and expand their financial performance.
Redfort RCM was built for the second category.
If you are evaluating your current revenue cycle and wondering whether hidden leakage exists that question alone is the signal.
It is time to audit structurally, not administratively.